- Medicines
- Personal Care
- Skin Cream
- Sunscreen
- Face Wash
- Skin and Body Soap
- Acne Care
- Body Lotions
- Moisturising Lotion
- Moisturising Cream
- Mosquito Repellent
- Moisturising Gel
- Body Wash
- Hair Oils
- Hair Shampoo
- Hair Conditioners
- Hair Supplements
- Hair Colour
- Hair Serum
- Hair Mask
- Hair Solutions
- Baby Diapers and Wipes
- Baby Lotion and Moisturising Cream
- Baby Bath Essentials
- Baby Skin Care
- Baby and Infant Food
- Baby Healthcare
- Women Multivitamins
- Ovulation Test Kit and Women Intimate Care
- Sanitary Pads
- Nutritional Drinks
- Condoms
- Lubricants
- Massage Gels
- Personal Body Massagers
- Men Performance Booster
- Sexual Health Supplements
- Massage Oils
- Ayurveda
- Tooth Paste
- Mouth Ulcer Gel
- Mouthwash
- Toothache and Gum Pain
- Tooth Brush
- Gargle Solution
- Orthopaedic Supports
- Adult Diapers
- Footwear
- Mobility and Support Accessories
- Urinary Support and Care
- Health Conditions
- Bone and Joint Care
- Digestive Care
- Eye Care
- Pain Relief
- Smoking Cessation
- Liver Care
- Stomach Care
- Cold and Cough
- Heart Care
- Kidney Care
- Piles, Fissures & Fistula
- Respiratory Care
- Mental Wellness
- Derma Care
- Pre and Probiotics
- Acidity
- Gas
- Constipation
- Loose Motion/Diarrhoea
- Digestive Fibres
- Digestive Enzymes
- Eye Lubricant Drops
- Lens Solution
- Safety Eye Wear
- Eye Cream
- Eye Vitamins and Supplements
- Eye Drops
- Eye Ointment and Gel
- Nicotine Patch
- Nicotine Gum
- Nicotine Lozenges
- Cough Syrups
- Chest Rubs and Balms
- Nasal Spray
- Lozenges
- Inhalant Capsules
- Cold and Cough Tablets
- Vitamins & Supplements
- Diabetes Care
- Healthcare Devices
- Homeopathic Medicine
- Health Guide
Peptic Ulcer
Peptic ulcer disease (PUD) is a condition characterised by open sores in the lining of the stomach, or duodenum, or lower oesophagus. It is commonly caused by Helicobacter pylori infection or long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs). Symptoms include burning or gnawing stomach pain, and treatment typically involves antibiotics, acid-reducing medications, and lifestyle changes.
Last updated on : 30 Apr, 2026
Read time : 14 mins

Overview of Disease
Peptic ulcer disease (PUD) is a common gastrointestinal disorder that affects millions of people worldwide. It occurs when the protective mucus layer of the stomach or duodenum is compromised, allowing the digestive acids to erode the lining and cause ulcers. In this article, we will explore the causes, symptoms, diagnosis, and treatment of peptic ulcers to provide a comprehensive overview of this prevalent gastrointestinal condition.
What is a Peptic Ulcer?
A peptic ulcer is an open sore that develops on the inner lining of the stomach (gastric ulcer) or the upper part of the small intestine, known as the duodenum (duodenal ulcer). These ulcers form when the protective mucus layer that shields the stomach and duodenum from digestive acids is weakened or breaks down, allowing the acids to eat away at the underlying tissue. Peptic ulcers can cause significant discomfort and may lead to complications if left untreated, making early diagnosis and appropriate treatment crucial.
Key Factors about Peptic Ulcer
| Category | Details |
| Also Referred to as | Stomach ulcer, gastric ulcer, duodenal ulcer, peptic ulcer disease |
| Commonly Occurs In | Adults, especially older adults, and those with H. pylori infection or NSAID use |
| Affected Organ | Stomach, duodenum (first part of the small intestine) |
| Type | Gastric ulcer (in the stomach), Duodenal ulcer (in the duodenum) |
| Common Signs | Burning stomach pain, nausea, bloating, belching, vomiting, and blood in the stool |
| Consulting Specialist | Gastroenterologist, General surgeon |
| Treatment Procedures | Medicines to reduce stomach acid, antibiotics for H. pylori, lifestyle changes, and surgery if necessary |
| Managed By | Antibiotics (Amoxicillin, Clarithromycin, Metronidazole & Tetracycline), Proton pump inhibitors (Omeprazole, Pantoprazole & Rabeprazole), H2-receptor antagonists (Famotidine & Nizatidine), Antacids, Surgery (Vagotomy, Ant |
| Mimicking Condition | Heartburn, indigestion, gastro-esophageal reflux disease (GERD) |
Types of Peptic Ulcer
The various types of peptic ulcers include:
- Gastric Ulcer: Gastric ulcers occur in the stomach lining. Symptoms may include pain that is exacerbated by eating and relieved by antacids. The pain pattern can be less consistent compared to duodenal ulcers.
- Duodenal Ulcer: Duodenal ulcers occur in the first part of the small intestine (duodenum). They are often associated with H. pylori infection and can cause pain that is relieved by eating and worsened by hunger.
- Oesophageal Ulcer: Oesophageal ulcers, though less common, occur in the lower oesophagus. They are often associated with gastroesophageal reflux disease (GERD) and can cause symptoms such as heartburn and difficulty swallowing.
Identifying the specific type of peptic ulcer is essential for determining the most effective treatment approach and managing potential complications.
Early Signs of Disease
The early signs of a peptic ulcer include:
- Dull or burning stomach pain that occurs between meals or at night and lasts from a few minutes to hours
- Feeling full quickly after eating only a small amount of food, indicating the ulcer may be affecting digestion
- Burping and indigestion, especially when accompanied by a gnawing sensation in the stomach
- Nausea and vomiting, which are common early signs if the ulcer is obstructing the digestive tract
- Unintentional weight loss that occurs due to reduced appetite or fear of eating because of pain
Symptoms of Peptic Ulcer
The symptoms of peptic ulcers can vary among individuals, but they commonly include the following:
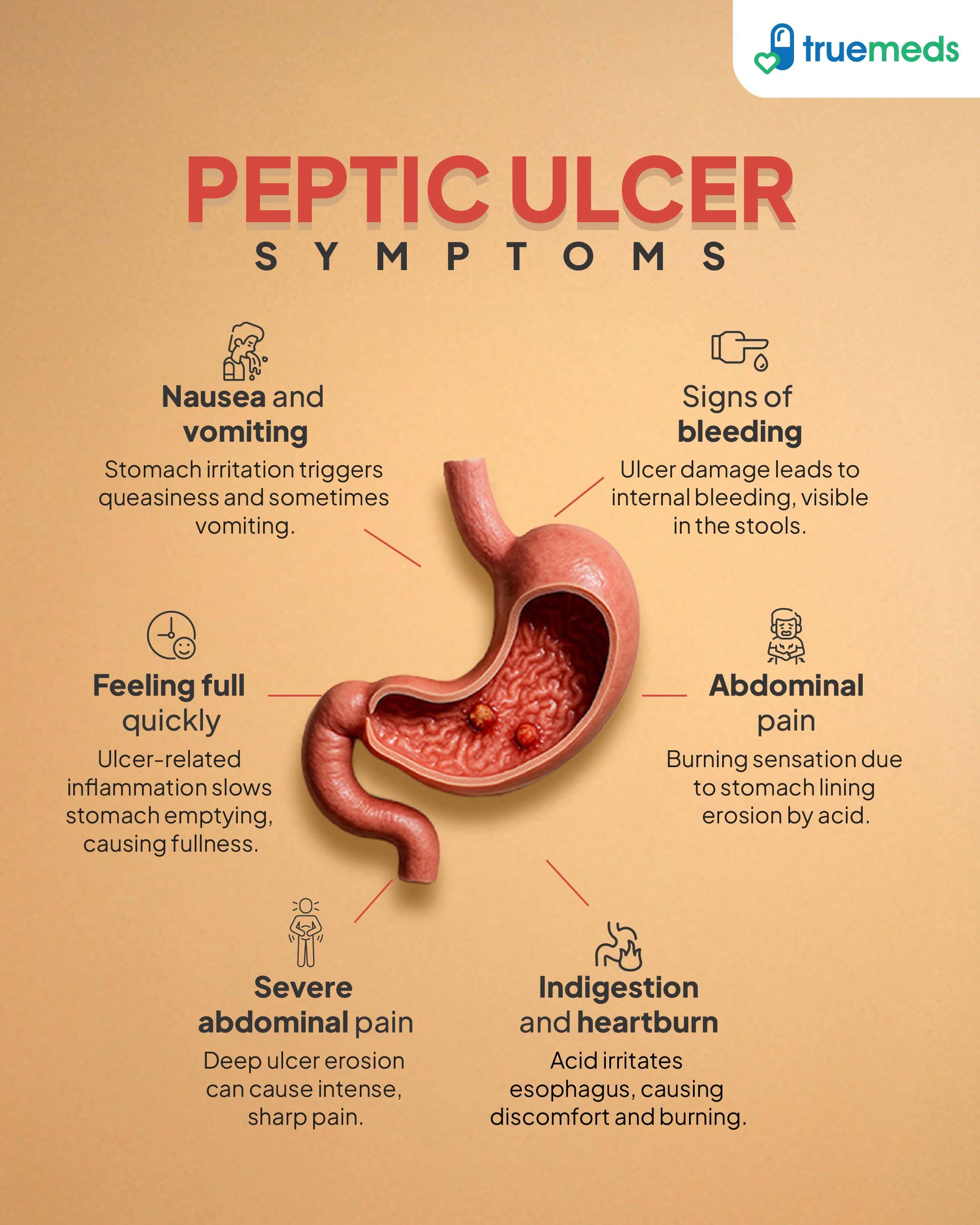
- Abdominal pain: Many individuals experience dull or burning pain located between the breastbone and the belly button, which typically occurs between meals or at night.
- Indigestion and heartburn: Patients often suffer from persistent indigestion and heartburn, which may worsen after consuming certain trigger foods.
- Nausea and vomiting: Intermittent nausea and vomiting may occur and may be temporarily relieved by food or antacids, particularly in duodenal ulcers.
- Feeling full quickly: Some individuals may notice sensations of feeling full quickly or bloated, particularly if the ulcer affects the duodenum.
- Signs of bleeding: Vomiting blood or passing black, tarry stools are alarming signs that indicate a bleeding ulcer requiring urgent medical care.
- Severe abdominal pain: Sudden and severe abdominal pain may suggest that an ulcer has perforated through the stomach or duodenal wall, signalling a medical emergency.
Stages of Peptic Ulcer
Peptic ulcer disease does not have a formal clinical staging system. Ulcers may be described as acute (newly formed) or chronic (long-standing or recurrent), but this classification is descriptive rather than a staged progression of disease. Chronic ulcers are more often associated with persistent H. pylori infection or ongoing NSAID use.
- Acute: Acute peptic ulcers are new and typically have a sudden onset. They are often associated with severe pain and, in some cases, bleeding. Acute ulcers can heal quickly if treated promptly, but they can also lead to complications such as perforation or obstruction if left untreated.
- Chronic: Chronic peptic ulcers are long-standing and may recur over time. They often result from persistent infection with H. pylori or continued use of NSAIDs. Chronic ulcers can lead to scarring and narrowing of the stomach or duodenum, which can cause complications like gastric outlet obstruction.
Causes of Peptic Ulcer
The most common causes of peptic ulcers include:
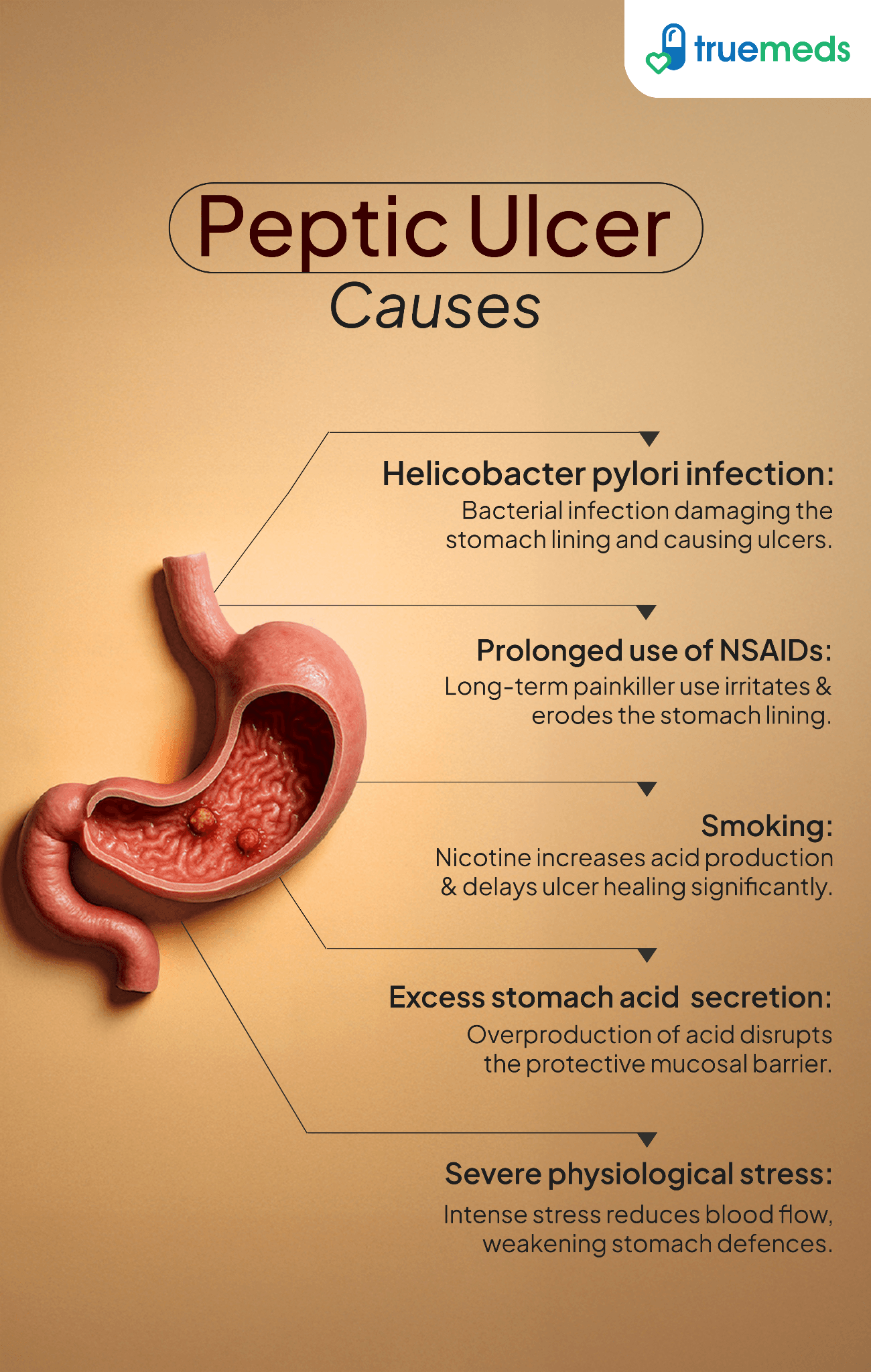
- Helicobacter pylori infection: Infection with the bacterium Helicobacter pylori (H. pylori) can damage the protective lining of the stomach and duodenum, leading to ulcer formation.
- Prolonged use of NSAIDs: The extended use of nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin, ibuprofen, and naproxen, can reduce the stomach's protective mucus layer, increasing the risk of ulcers.
- Excess stomach acid secretion: This can occur due to gastrinomas, which are tumours that secrete excessive amounts of gastrin, leading to increased acid production.
- Severe physiological stress: High levels of stress, such as from surgery, trauma, or serious illness, can contribute to ulcer formation.
- Smoking: Tobacco use can increase stomach acid production and reduce the effectiveness of the stomach's protective mechanisms, leading to a higher risk of ulcer development.
Risk Factors
Several factors can increase the likelihood of developing these ulcers, including:
- Frequent use of NSAIDs, especially at high doses and long durations
- H. pylori infection (ACG, 2022)
- Smoking increases ulcer risk and impairs healing. Alcohol does not directly cause ulcers but may irritate the gastric mucosa and worsen symptoms.
- Age over 50 years old
- Family history of peptic ulcers
- Serious illness or physical trauma
- Radiation treatment to the abdomen
Who's at Risk?
Certain populations are more at risk for developing peptic ulcers, including:
- People who frequently use NSAIDs for pain relief from conditions like arthritis
- Those living in areas with high rates of H. pylori infection
- Older adults over age 50
- Smokers and heavy alcohol drinkers
- Individuals with a family history of ulcers
- People under extreme physiological stress
- Those undergoing radiation therapy targeting the abdomen
Understanding personal risk helps with the prevention and early detection of peptic ulcers through lifestyle changes and regular check-ups.
Complications
Peptic ulcers can lead to several serious complications if not properly managed. Some of the potential complications include:
- Haemorrhage or bleeding: The most common complication occurs when the ulcer erodes into a blood vessel, resulting in bleeding. Symptoms include vomiting blood or coffee-ground material, passing black, tarry stools, and signs of blood loss such as weakness, dizziness, and pale skin.
- Perforation: This serious complication arises when the ulcer creates a hole in the stomach or duodenum wall, allowing bacteria and partially digested food to leak into the abdominal cavity. This can cause peritonitis, a life-threatening infection. Symptoms include sudden, severe abdominal pain and signs of infection, such as fever and abdominal rigidity.
- Penetration: In some cases, the ulcer may penetrate the wall of the stomach or duodenum but remain contained by adhesions or nearby organs. This is known as penetration or confined perforation, with symptoms including intense, persistent pain that may radiate to the back.
- Gastric outlet obstruction: This complication occurs when inflammation or scarring from the ulcer narrows the opening between the stomach and small intestine, preventing food from passing through. Symptoms include repeated vomiting of undigested food, bloating, early satiety, and unintentional weight loss.
Prevention of Peptic Ulcer
Preventing peptic ulcers involves addressing common causes and risk factors. Some of the preventative measures include:
- Avoiding NSAIDs: One key strategy is to limit the long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs), as these can damage the stomach lining.
- Eradicating H. pylori: Another important preventive measure is the eradication of Helicobacter pylori (H. pylori) infection, a major cause of peptic ulcers. Treatment typically involves a combination of antibiotics and proton pump inhibitors (PPIs) to eliminate the bacteria and reduce stomach acid production.
- Healthy lifestyle choices: Maintaining a healthy diet and managing stress can be beneficial. Additionally, avoiding smoking and excessive alcohol consumption can help reduce the risk of developing peptic ulcers.
Diagnosis & Tests
Diagnosing peptic ulcers involves a combination of medical history, physical examination, and diagnostic tests. The most common tests used to diagnose peptic ulcers include:
- Upper gastrointestinal (GI) endoscopy: This procedure involves inserting a flexible tube with a camera (endoscope) down the throat and into the stomach and duodenum. The endoscope allows the doctor to visualise the ulcer and take a biopsy if necessary.
- Barium swallow or upper GI series: In this test, the patient drinks a chalky liquid containing barium, which coats the lining of the digestive tract. X-rays are then taken to visualise the stomach and duodenum, revealing any ulcers or abnormalities.
- Urea breath test or stool antigen test: These tests are used to detect the presence of H. pylori bacteria. The urea breath test involves drinking a solution containing urea labelled with carbon-13, which the bacteria break down, releasing labelled carbon dioxide that can be detected in the breath. The stool antigen test detects H. pylori proteins in a stool sample (Malik et al., 2024).
- Blood tests: While blood tests cannot directly diagnose peptic ulcers, they can check for anaemia (a sign of bleeding) and test for H. pylori antibodies, indicating a current or past infection.
Treatment & Management
The management of peptic ulcer disease involves several treatment options customised to the specific cause and complications of the ulcer. The treatment options include:
1. H. pylori-Induced Ulcers
Peptic ulcers caused by Helicobacter pylori (H. pylori) infection require a targeted treatment approach to eradicate the bacteria and promote ulcer healing. In many regions, bismuth-based quadruple therapy is recommended as first-line treatment because of increasing clarithromycin resistance. Triple therapy may still be used where clarithromycin resistance rates are low (ACG, 2022). The prescribed antibiotics include Amoxicillin, Clarithromycin, Metronidazole, Tinidazole, and Tetracycline, which work synergistically to eliminate H. pylori. In some cases, quadruple therapy, which includes a bismuth-containing compound, may be recommended for treatment-resistant infections.
2. NSAID-Induced Ulcers
Long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs) can damage the stomach lining, leading to ulcers. The first step in treatment is discontinuing NSAID use whenever possible. If the patient requires continued NSAID therapy for pain or inflammation management, PPIs such as Pantoprazole and Omeprazole are prescribed to reduce gastric acid secretion and prevent further mucosal damage. Additionally, alternative medications like COX-2 inhibitors may be considered, as they pose a lower risk of gastric ulcer formation (NICE, 2023).
3. Second-Line Therapies
For patients who fail initial H. pylori treatment, sequential or quadruple therapy is recommended. Quadruple therapy typically includes a PPI, two antibiotics, and a bismuth compound, enhancing bacterial eradication rates. Non-bismuth-based sequential therapy follows a stepwise approach, first administering a PPI and amoxicillin, followed by a PPI combined with clarithromycin and metronidazole or tinidazole. These alternative regimens increase effectiveness, especially in cases where bacterial resistance to standard antibiotics is a concern.
4. Bleeding Ulcers
Bleeding peptic ulcers are a medical emergency requiring immediate intervention. Initial treatment involves intravenous (IV) PPI therapy, which stabilises the clot and reduces gastric acid to prevent further bleeding. Endoscopic therapy is the preferred approach to achieve hemostasis, using techniques such as thermal coagulation, injection therapy, or hemoclips to control bleeding at the ulcer site. If endoscopic treatment is unsuccessful, angiographic embolisation or surgical intervention may be required to manage persistent haemorrhage.
5. Perforation or Stenosis
Perforated ulcers, where the ulcer erodes completely through the stomach or duodenal wall, can lead to life-threatening peritonitis. Stenosis, or narrowing of the gastric outlet, occurs due to chronic ulceration and scarring. These conditions often require surgical intervention, particularly if perforation leads to peritoneal contamination or if stenosis causes severe obstruction. Surgery may involve simple closure of the perforation, gastric resection, or bypass procedures, depending on the severity. In mild cases, conservative management with IV PPIs, nasogastric decompression, and close monitoring may be attempted.
6. Maintenance Therapy
To prevent ulcer recurrence, especially in high-risk patients, long-term PPI therapy is recommended. Patients who cannot tolerate PPIs or require alternative options may use histamine 2-receptor antagonists H2RAs such as Famotidine or Nizatidine (Ranitidine is no longer recommended due to withdrawal from many markets), which work by inhibiting histamine-induced acid secretion. Maintenance therapy is particularly crucial for individuals who have a history of recurrent ulcers, require long-term NSAID or aspirin therapy, or have persistent H. pylori infections.
7. Symptomatic Relief & Ulcer Protection
For immediate symptom relief and gastric mucosal protection, additional medications are used alongside primary treatment strategies. Antacids such as Sodium Bicarbonate, Magnesium Hydroxide, Aluminium Hydroxide, and Magaldrate neutralise stomach acid and provide rapid relief from ulcer-related pain and discomfort. Ulcer protectives like Sucralfate and Colloidal Bismuth form a protective barrier over the ulcer, promoting healing and preventing further irritation from gastric acids. Anticholinergics, including Pirenzepine and Oxyphenonium, help reduce acid secretion by blocking vagal stimulation, thereby aiding ulcer healing. These medications complement primary treatment approaches and enhance overall patient recovery.
When to See a Doctor?
It is essential to seek medical attention if you experience symptoms of a peptic ulcer, such as persistent stomach pain, nausea, vomiting, or dark stools. If left untreated, peptic ulcers can lead to serious complications like bleeding, perforation, or obstruction. You should also consult a doctor if you have a history of peptic ulcers and are taking NSAIDs or low-dose aspirin, as these medications can increase the risk of ulcer recurrence.
Key Takeaways
- Peptic ulcers are sores that develop in the lining of the stomach or duodenum, often caused by H. pylori infection or prolonged use of NSAIDs.
- Common symptoms include abdominal pain, nausea, vomiting, and unintentional weight loss.
- Diagnosis involves a combination of tests, such as endoscopy, biopsy, and breath or stool tests for H. pylori.
- Treatment typically involves a combination of antibiotics and acid-reducing medications, such as proton pump inhibitors.
- Lifestyle modifications, including avoiding NSAIDs, quitting smoking, and managing stress, can help prevent peptic ulcers and promote healing.
- Seek medical attention if you experience symptoms suggestive of a peptic ulcer or if your diagnosed ulcer does not improve with treatment.
FAQs
Who has the highest risk of developing peptic ulcers?
Do peptic ulcers go away on their own?
Is milk good for an ulcer?
How can I heal my ulcer myself?
What should be avoided when dealing with a peptic ulcer?
What lifestyle factors cause peptic ulcers?
What are the home remedies for peptic ulcers?
Can peptic ulcers be cured with ayurveda?
References
- American College of Gastroenterology (ACG). (2022). ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. https://doi.org/10.14309/ajg.0000000000002010
- Malfertheiner, P., et al. (2022). Management of Helicobacter pylori infection — Maastricht VI/Florence Consensus. Gut, 71(9), 1724–1762.
https://doi.org/10.1136/gutjnl-2022-327745 - National Institute for Health and Care Excellence (NICE). (2023). Peptic ulcer disease: Assessment and management. https://www.nice.org.uk/guidance/cg184/ifp/chapter/peptic-ulcer
- Malik, T. F., Gnanapandithan, K., & Singh, K. (2026). Peptic ulcer disease. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK534792/

Check Related Salts
Browse Other Conditions
Latest health articles
Top Health Essentials






























Disclaimer
Top-Selling Medicines:
...View more
Top-OTC medicines:
...View more
Company
About UsHealth ArticleHealth StoriesHealth LibraryDiseases & Health ConditionsAyurvedaUnderstanding Generic MedicinesAll MedicinesAll BrandsNeed HelpFAQSecuritySavings CalculatorAdvertise with UsSubscribe
Registered Office Address
Grievance Officer
Download Truemeds
Contact Us
Our customer representative team is available 7 days a week from 9 am - 9 pm.
v4.28.0
2026 - Truemeds | All rights reserved. Our content is for informational purposes only. See additional information.
Our Payment Partners

