- Medicines
- Personal Care
- Skin Cream
- Sunscreen
- Face Wash
- Skin and Body Soap
- Acne Care
- Body Lotions
- Moisturising Lotion
- Moisturising Cream
- Mosquito Repellent
- Moisturising Gel
- Body Wash
- Hair Oils
- Hair Shampoo
- Hair Conditioners
- Hair Supplements
- Hair Colour
- Hair Serum
- Hair Mask
- Hair Solutions
- Baby Diapers and Wipes
- Baby Lotion and Moisturising Cream
- Baby Bath Essentials
- Baby Skin Care
- Baby and Infant Food
- Baby Healthcare
- Women Multivitamins
- Ovulation Test Kit and Women Intimate Care
- Sanitary Pads
- Nutritional Drinks
- Condoms
- Lubricants
- Massage Gels
- Personal Body Massagers
- Men Performance Booster
- Sexual Health Supplements
- Massage Oils
- Ayurveda
- Tooth Paste
- Mouth Ulcer Gel
- Mouthwash
- Toothache and Gum Pain
- Tooth Brush
- Gargle Solution
- Orthopaedic Supports
- Adult Diapers
- Footwear
- Mobility and Support Accessories
- Urinary Support and Care
- Health Conditions
- Bone and Joint Care
- Digestive Care
- Eye Care
- Pain Relief
- Smoking Cessation
- Liver Care
- Stomach Care
- Cold and Cough
- Heart Care
- Kidney Care
- Piles, Fissures & Fistula
- Respiratory Care
- Mental Wellness
- Derma Care
- Pre and Probiotics
- Acidity
- Gas
- Constipation
- Loose Motion/Diarrhoea
- Digestive Fibres
- Digestive Enzymes
- Eye Lubricant Drops
- Lens Solution
- Safety Eye Wear
- Eye Cream
- Eye Vitamins and Supplements
- Eye Drops
- Eye Ointment and Gel
- Nicotine Patch
- Nicotine Gum
- Nicotine Lozenges
- Cough Syrups
- Chest Rubs and Balms
- Nasal Spray
- Lozenges
- Inhalant Capsules
- Cold and Cough Tablets
- Vitamins & Supplements
- Diabetes Care
- Healthcare Devices
- Homeopathic Medicine
- Health Guide
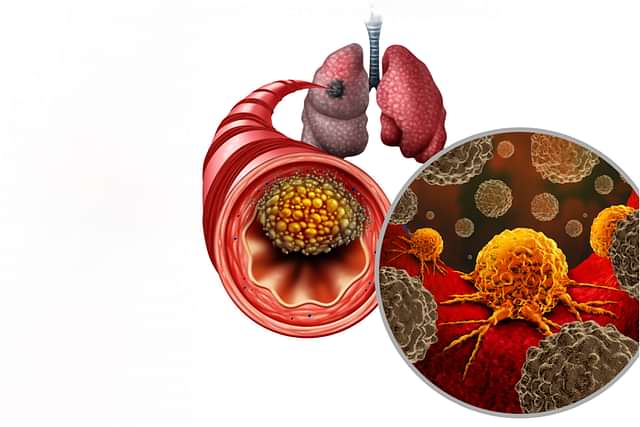
Non Small Cell Lung Cancer
Non-small cell lung cancer (NSCLC) is the most common category of lung cancer, accounting for the majority of lung cancer cases (approximately 80–85%). NSCLC comprises several histologic subtypes, most commonly adenocarcinoma, squamous cell carcinoma, and large-cell (undifferentiated) carcinoma and, increasingly, the management is driven by both histology and molecular alterations (EGFR, ALK, ROS1, BRAF, MET, RET, NTRK, KRAS, etc.). Staging (TNM) and molecular profiling guide prognosis and treatment selection (NCCN (2024)). Treatment and prognosis for NSCLC depend on the stage of the cancer, which is determined by the extent of its spread.
Last updated on : 29 Apr, 2026
Read time : 16 mins
Overview of Disease
Non-small cell lung cancer (NSCLC) is a serious and potentially life-threatening condition that affects a significant number of people worldwide. As a type of lung cancer that originates in the tissues of the lung, NSCLC is distinguished from small cell lung cancer (SCLC) by its cellular characteristics and growth patterns. This article aims to provide a comprehensive overview of non-small cell lung cancer, including its definition, stages, and prognosis.
What is Non Small Cell Lung Cancer?
NSCLC denotes a group of epithelial lung cancers that are biologically and clinically distinct from small-cell lung cancer (SCLC). Beyond histology (adenocarcinoma, squamous cell carcinoma, large-cell carcinoma and rarer subtypes), molecular driver alterations now play a central role in diagnosis and treatment selection for advanced disease. Distinguishing NSCLC from SCLC is essential because treatment pathways, systemic agents, and prognosis differ markedly between the two.
Key Factors about Non Small Cell Lung Cancer
| Category | Details |
| Also Referred to as | Bronchogenic carcinomas, NSCLC |
| Commonly Occurs In |
|
| Affected Organ | Lungs (bronchial tree, alveolar tissue). Common metastatic sites include the brain, bones, liver, and adrenal glands; lymph node involvement (intrapulmonary, hilar, mediastinal) influences staging and treatment planning. Cutaneous metastases are uncommon. |
| Type | Adenocarcinoma, Squamous cell carcinoma, Large cell carcinoma |
| Common Signs |
|
| Consulting Specialist | Pulmonologist, Oncologist |
| Treatment Procedures | Surgery, Chemotherapy, Immunotherapy, Targeted therapy, Radiation therapy |
| Managed By |
|
| Mimicking Condition | Common illnesses or effects of long-term smoking, chronic obstructive pulmonary disease (COPD), pneumonia |
Types of Non Small Cell Lung Cancer
Non-small cell lung cancer is categorised into several subtypes based on the appearance of the tumour cells under a microscope. The main non-small cell lung cancer subtypes include:
- Adenocarcinoma: This is the most common subtype of NSCLC, starting in the cells that line the alveoli (tiny air sacs) in the lungs, where oxygen enters the blood and carbon dioxide leaves it. Adenocarcinoma is found in both smokers and non-smokers and is more common in women and younger individuals.
- Squamous cell carcinoma: This type develops in the flat cells that cover the surface of the airways in the lungs. It is more commonly associated with smoking and tends to be located near the centre of the lungs, near a main airway (the bronchus).
- Large cell carcinoma: The cancer cells appear larger than typical cells under the microscope. This type can occur in any part of the lung and tends to grow and spread quickly, making it harder to treat.
- Sarcomatoid carcinoma: This is a rare subtype of NSCLC that can be aggressive and difficult to treat. It can occur in any part of the lung and can have varying growth rates.
- Adenosquamous carcinoma: This is a less common subtype of NSCLC that contains elements of both adenocarcinoma and squamous cell carcinoma.
- Molecular subgroups: For therapeutic decision-making in advanced NSCLC, identifying molecular drivers (e.g., EGFR mutation, ALK or ROS1 rearrangement, BRAF V600E, MET exon 14 skipping, RET fusions, NTRK fusions, and KRAS G12C) and assessing PD-L1 expression are standard of care, because they directly determine targeted therapy and immunotherapy choices.
Symptoms of Non Small Cell Lung Cancer
The symptoms of non-small cell lung cancer can vary depending on the stage and location of the cancer within the lungs. Common symptoms include:
- Chest pain: Individuals may experience persistent chest pain that can be sharp or dull, often worsening with deep breaths or coughing. This discomfort can indicate underlying issues in the lungs or surrounding tissues.
- Persistent cough: A cough that does not go away or worsens over time can be a significant warning sign. It may be dry or produce mucus, leading to concerns about lung health.
- Coughing up blood: Haemoptysis, or coughing up blood, is a concerning symptom that should prompt immediate medical evaluation. This can indicate irritation or damage in the respiratory tract, potentially linked to cancer.
- Fatigue: Patients may experience extreme fatigue that is not relieved by rest, impacting daily activities. This persistent tiredness can be a result of the body's energy being diverted to the disease process.
- Loss of appetite: A noticeable decrease in appetite can occur, often accompanied by feelings of nausea or aversion to food. This symptom can lead to further weight loss and nutritional deficiencies.
- Unintended weight loss: Unexplained weight loss can be alarming and may be an indicator of cancer progression. It often results from a combination of loss of appetite and increased metabolic demands due to the disease.
- Shortness of breath: Many patients experience increasing difficulty in breathing, which may occur even at rest. This can be caused by tumour growth obstructing airways or fluid accumulation in the lungs.
- Wheezing: A wheezing sound during breathing can signal narrowed airways, which might be due to tumours or inflammation. This symptom can make breathing challenging, especially during physical activity.
- Hoarseness: Changes in voice or persistent hoarseness can result from pressure on the laryngeal nerve. This symptom may signal nearby tumour growth and should be evaluated by a doctor.
- Nail problems: Changes in the appearance of nails, such as clubbing or discolouration, can occur in response to lung cancer. These changes may reflect underlying respiratory or circulatory issues.
- Swallowing difficulty: Dysphagia, or difficulty swallowing, can arise if the tumour presses on the oesophagus or related structures. This can lead to choking hazards and nutritional complications.
Stages of Non Small Cell Lung Cancer
NSCLC is staged using the TNM system (Tumour size/extent — T, regional lymph node involvement — N, and distant metastasis — M) from the IASLC/AJCC 8th edition. Accurate staging requires CT chest/abdomen and PET-CT in most cases, plus brain MRI for candidates for curative therapy or symptomatic patients. Key points:
- Stage 0 (in situ / AIS): carcinoma in situ or adenocarcinoma in situ (tumour confined to the epithelium).
- Stage I (IA1, IA2, IA3, IB): small tumours confined to the lung without nodal involvement — further subdivided by tumour size (e.g., IA1 ≤1 cm, IA2 >1–2 cm, IA3 >2–3 cm, IB >3–4 cm depending on 8th edition criteria).
- Stage II (IIA, IIB): larger primary tumours and/or ipsilateral peribronchial or hilar nodal disease (N1), or primary tumours with features that increase risk locally.
- Stage III (IIIA, IIIB, IIIC): locally advanced disease with ipsilateral or contralateral mediastinal nodal involvement and/or invasion of central structures; these subcategories reflect combinations of T and N descriptors and are heterogeneous — management is multidisciplinary (surgery, chemoradiation, or combined modalities).
- Stage IV (M1a, M1b, M1c): distant metastases to other organs (brain, bone, liver, adrenal, etc.) or malignant pleural/pericardial effusion.
Note: The TNM system uses multiple size cutoffs and descriptors — for patient care, use institutional staging reference or an up-to-date TNM table (IASLC/AJCC 8th edition) and perform staging in a multidisciplinary tumour board.
Causes of Non Small Cell Lung Cancer
While the exact cause of non-small cell lung cancer is not known, several risk factors have been identified. These include:
- Smoking: Smoking is a major risk factor for non-small cell lung cancer, with many people diagnosed having a history of smoking. The risk increases with the number of cigarettes smoked and the duration of smoking.
- Exposure to carcinogens: Exposure to certain carcinogens, such as asbestos, radon, and arsenic, can increase the risk of developing NSCLC. Occupational exposure to these substances, as well as air pollution, may contribute to the development of lung cancer.
- Genetic/molecular alterations: Mutations and rearrangements such as EGFR, ALK, ROS1, BRAF V600E, MET exon 14 skipping, RET fusions, NTRK fusions, and KRAS G12C are typically acquired somatic alterations that drive tumour growth and are key therapeutic targets in NSCLC. Germline (inherited) mutations are much less commonly the cause of NSCLC. Risk factors such as tobacco smoke, radon, and occupational carcinogens contribute to mutagenesis.
Risk Factors
- Smoking
- Exposure to secondhand smoke
- Exposure to other carcinogens (such as asbestos, arsenic, chromium, beryllium, nickel, soot, tar, diesel exhaust, and other chemicals)
- Radon exposure
- Air pollution
- Family history
- Previous radiation therapy to the chest for other cancers
- Inherited gene changes, such as mutations in genes like CHEK2, ATM, TP53, BRCA1, EGFR, APC, and PALB2
Prevention of Non Small Cell Lung Cancer
Preventing non-small cell lung cancer involves reducing exposure to known risk factors and adopting healthy lifestyle choices. Some of the preventive measures include:
- Avoid tobacco smoke: Quit smoking and avoid exposure to secondhand smoke. This is the most effective way to reduce the risk of non-small cell lung cancer.
- Reduce exposure to carcinogens: Limit exposure to radon by testing your home and workplace and taking steps to reduce radon levels if necessary. Additionally, minimise exposure to occupational carcinogens by following safety guidelines and wearing protective equipment.
- Maintain a healthy diet: Eating a diet rich in fruits and vegetables may help lower the risk of NSCLC. Avoid taking beta-carotene supplements, especially if you are a smoker, as they have been linked to an increased risk of lung cancer.
- Exercise regularly: Engaging in regular physical activity can help maintain overall health and potentially reduce the risk of developing non-small cell lung cancer.
- Screening: Low-dose CT (LDCT) screening for high-risk individuals (longstanding heavy smokers or those meeting local guideline criteria) reduces lung cancer mortality and is recommended by many guideline bodies; implement this per local/national screening programmes and eligibility criteria. Smoking cessation remains the single most effective prevention measure.
Diagnosis & Tests
If a person experiences symptoms suggestive of non-small cell lung cancer, such as persistent cough, chest pain, shortness of breath, or unexplained weight loss, their doctor may recommend various diagnostic tests to determine the cause. The tests may include:
- Physical examination: A thorough physical exam, including an assessment of the patient's medical history and risk factors, can provide initial insights into their condition.
- Imaging: Contrast-enhanced CT chest ± abdomen and FDG PET-CT (for systemic staging) are standard for staging. Brain MRI with contrast is recommended for staging in patients with suspected advanced disease or those being considered for curative treatment. A chest X-ray is not sufficient for staging.
- Tissue diagnosis: Histologic/cytologic confirmation by bronchoscopic biopsy, CT-guided percutaneous biopsy, or surgical biopsy is required. Obtain sufficient tissue for both histology and comprehensive molecular testing.
- Molecular testing and PD-L1: For all patients with advanced (metastatic) non-small cell lung cancer, broad molecular profiling (NGS panel where available) for driver alterations (EGFR, ALK, ROS1, BRAF, MET, RET, NTRK, KRAS, etc.) and PD-L1 immunohistochemistry is standard of care because results determine targeted therapy and immunotherapy options. Liquid biopsy (ctDNA) can be used when tissue is inadequate (NCCN, 2024).
- Additional tests: Pulmonary function tests for surgical candidates; mediastinal staging (EBUS/EUS ± mediastinoscopy) when nodal disease is suspected; pleural fluid cytology if an effusion is present.
Treatment & Management
Management is stage-dependent and increasingly biomarker-driven. For early-stage disease (I–II), surgery with curative intent (lobectomy preferred) ± adjuvant chemotherapy/targeted therapy is standard. For medically inoperable early-stage tumours, SBRT is a curative option. Locally advanced stage III disease often requires multimodality therapy (concurrent chemoradiation and consolidation immunotherapy for unresectable stage III). Metastatic (stage IV) disease is generally treated with systemic therapy directed by histology, PD-L1 status, and actionable driver mutations (targeted therapy/immunotherapy ± chemotherapy). Palliative and supportive care should be integrated at all stages.
1. Surgery
Anatomic lobectomy with systematic lymph node sampling is the standard surgical approach for fit patients with operable early-stage NSCLC. Sublobar resection (segmentectomy or wedge) may be appropriate for very small tumours or patients with limited pulmonary reserve. Pneumonectomy is reserved for extensive central disease not amenable to lesser resections.
Adjuvant therapy: Adjuvant platinum-based chemotherapy is indicated for selected stage II–IIIa patients; for resected EGFR-mutant stage IB–IIIa disease, adjuvant osimertinib for 3 years is recommended based on randomized trial data (ADAURA) and guideline updates (Wu et al., 2020).
2. Radiation Therapy
High-energy rays target cancer cells, often used in medically inoperable early-stage NSCLC. Stereotactic body radiation therapy (SBRT) provides high local control rates and is an accepted curative option. SBRT is also used for oligometastatic disease in selected patients. Consolidation immunotherapy (durvalumab) after concurrent chemoradiation is standard for unresectable stage III NSCLC with no contraindications.
Types include:
- External Beam Radiation Therapy (EBRT)
- Stereotactic Body Radiation Therapy (SBRT)
- Brachytherapy (internal radiation)
3. Chemotherapy
Platinum-based doublets remain a backbone for systemic therapy when targeted therapy is not indicated. Typical regimens include:
- Non-squamous NSCLC: cisplatin/carboplatin + pemetrexed (preferred non-squamous partner).
- Squamous NSCLC: cisplatin/carboplatin + gemcitabine or taxane (paclitaxel/docetaxel) are commonly used.
- Second-line/advanced options: docetaxel, gemcitabine, pemetrexed (where histology appropriate), or taxanes can be used depending on prior therapy. Other agents (etoposide, irinotecan) have limited routine use in NSCLC and are used selectively. Choice depends on histology, performance status, prior therapy, and presence of targetable mutations.
4. Targeted Therapy
Targeted agents are selected according to the specific genomic alteration: e.g., EGFR mutations — first/second/third-generation EGFR TKIs (osimertinib is favored in many settings); ALK rearrangements — alectinib, brigatinib, lorlatinib (depending on line and resistance profile); ROS1 — entrectinib or crizotinib; BRAF V600E — dabrafenib + trametinib; MET exon 14 skipping — capmatinib or tepotinib; RET fusions — selpercatinib or pralsetinib; NTRK fusions — larotrectinib or entrectinib; KRAS G12C — sotorasib/adagrasib in appropriate settings. Use guideline-recommended sequencing and testing to select therapy.
5. Immunotherapy
Immunotherapy enhances the body’s immune system to recognise and attack cancer cells. It's especially effective in patients whose tumours express high levels of PD-L1 or after chemotherapy failure.
The role of immune checkpoint inhibitors depends on the PD-L1 tumour proportion score (TPS) and prior therapy. Examples and typical uses:
- High PD-L1 (TPS ≥50%) without actionable driver mutation: pembrolizumab monotherapy is a standard first-line option.
- Lower PD-L1 or unselected patients: PD-1/PD-L1 inhibitors in combination with platinum-based chemotherapy (e.g., pembrolizumab + platinum doublet) are standard first-line regimens for many patients without driver mutations.
- Second-line / previously treated disease: nivolumab or atezolizumab may be used depending on prior therapies and approvals.
- Locally advanced unresectable stage III: consolidation durvalumab after concurrent chemoradiation improves progression-free and overall survival (PACIFIC regimen).
- Other agents: cemiplimab is an approved PD-1 inhibitor for certain PD-L1 high tumours, and other agents (atezolizumab) have specific indications and combinations. Treatment choice should follow the latest guideline algorithms and consider PD-L1, driver mutation status, comorbidity, and patient preference (Reck et al., 2021).
6. Supportive & Palliative Care
Focused on symptom management, enhancing quality of life, and addressing complications.
- Pain management: Analgesics, opioids
- Dyspnea relief: Bronchodilators, corticosteroids
- Procedures:
- Laser therapy, cryotherapy, and stent placement for airway obstruction
- Thoracentesis for pleural effusion
- Bone metastases: Bone-targeting agents (zoledronic acid or denosumab) reduce skeletal-related events and may help with pain control; incorporate with appropriate calcium/vitamin D supplementation and dental evaluation before therapy
- Nutritional and psychological support, physical therapy, and palliative counselling
Living with Disease
Living with NSCLC can be challenging, but there are several ways to manage the disease and maintain a good quality of life. Here are a few points to consider:
- Regular follow-up appointments with your doctor are crucial to monitor for any signs of recurrence or metastasis.
- Managing symptoms such as pain, shortness of breath, and fatigue is important for maintaining quality of life. This can involve medications, physical therapy, and supportive care.
- Quit smoking if you have not already, as it can improve treatment outcomes and reduce the risk of recurrence.
- Maintain a healthy lifestyle, including a balanced diet, regular exercise, and stress management techniques.
- Seek support from family, friends, or support groups to help cope with the emotional and psychological challenges of living with NSCLC.
When to See a Doctor?
If you experience any symptoms that concern you, such as a persistent cough, chest pain, shortness of breath, unexplained weight loss, or fatigue, it's important to consult your doctor promptly. For those undergoing treatment for non-small cell lung cancer, report any new or worsening symptoms to your doctor, as they may indicate a change in your condition or a need for adjustments in your treatment plan.
Key Takeaways
- Non-small cell lung cancer (NSCLC) is a complex disease that requires a multidisciplinary approach to treatment and management.
- The prognosis and survival rates for NSCLC depend on various factors, including the stage of the cancer, the patient's overall health, and the presence of specific genetic mutations.
- Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, and immunotherapy.
- Living with NSCLC can be challenging, but with proper care, support, and a healthy lifestyle, patients can maintain a good quality of life.
- Regular check-ups and early detection are crucial for improving the prognosis and effectively managing the disease.
- Five-year relative survival varies strongly by stage. Contemporary registry data (SEER/ACS) report approximately >60% 5-year relative survival for localised NSCLC, around 40% for regional disease, and approximately 10–15% for distant/metastatic disease, although exact figures depend on year, population, and evolving treatments. Use local registry data for region-specific figures.
FAQs
What is the survival rate for non-small cell lung cancer?
The 5-year survival rate for non-small cell lung cancer (NSCLC) varies based on the stage at diagnosis, ranging from 60-65% for localised NSCLC to 6-9% for distant NSCLC.
Is non-small cell carcinoma curable?
Early-stage non-small cell lung carcinoma has a higher chance of being cured with appropriate treatment. Advanced stages are often managed as a chronic condition.
What is a non-small cell lung cancer?
Non-small cell lung cancer (NSCLC), the most common type of lung cancer, is characterised by the appearance of cells under a microscope and includes subtypes like adenocarcinoma and squamous cell carcinoma.
Which is more treatable, small cell or non-small cell lung cancer?
Non-small cell lung cancer is generally more treatable than small cell lung cancer, especially when diagnosed early, as it grows slower and is more likely to be localised.
What are the warning signs of non-small cell lung cancer?
Warning signs of non-small cell lung cancer include persistent coughing, coughing up blood, chest pain that worsens with breathing or coughing, hoarseness, and weight loss.
What is the most aggressive lung cancer?
Small cell lung cancer (SCLC) is more aggressive than non-small cell lung cancer, typically requiring chemotherapy and radiation therapy and having lower overall survival rates.
What is the treatment of choice for non-small cell lung cancer?
Treatment for non-small cell lung cancer depends on the stage and may include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these methods.
How fast does non-small cell lung cancer spread without treatment?
What is the latest treatment for NSCLC?
What is the life expectancy with non-small cell lung cancer?
References
- National Comprehensive Cancer Network. (2024). NCCN Clinical Practice Guidelines in Oncology: Non–Small Cell Lung Cancer (Version 4.2024). NCCN. Available at https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450
- Ettinger, D. S., Wood, D. E., Aisner, D. L., et al. (2024). Non-Small Cell Lung Cancer, Version 4.2024, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network, 22(4), 249–317. https://doi.org/10.6004/jnccn.2204.0023
- Wu, Y.-L., et al. (2020). Osimertinib in resected EGFR-mutated non small-cell lung cancer (ADAURA). New England Journal of Medicine, 383, 1711–1723. https://doi.org/10.1056/NEJMoa2027071
- Tsuboi, M., et al. (2023). Overall survival with osimertinib in resected EGFR-mutated non-small-cell lung cancer. New England Journal of Medicine, 389, 113–127. https://doi.org/10.1056/NEJMoa2304594
- Reck, M., et al. (2021). Five-year outcomes with pembrolizumab versus chemotherapy for previously untreated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-024). Journal of Clinical Oncology, 39(13), 1298–1300. https://doi.org/10.1200/JCO.21.00174
Check Related Salts
Latest health articles

Top Health Essentials






























Disclaimer
Top-Selling Medicines:
...View more
Top-OTC medicines:
...View more
Company
About UsHealth ArticleHealth StoriesHealth LibraryDiseases & Health ConditionsAyurvedaUnderstanding Generic MedicinesAll MedicinesAll BrandsNeed HelpFAQSecuritySavings CalculatorAdvertise with UsSubscribe
Registered Office Address
Grievance Officer
Download Truemeds
Contact Us
Our customer representative team is available 7 days a week from 9 am - 9 pm.
v4.28.5
2026 - Truemeds | All rights reserved. Our content is for informational purposes only. See additional information.
Our Payment Partners

